
Reaching for something on a high shelf produces a sharp catch of pain. Lifting the arm overhead becomes difficult. Sleeping on that side is no longer possible. And when asked what happened, many patients say the same thing: nothing happened. There was no fall, no accident, no specific moment they can point to.
This is one of the most common presentations of a rotator cuff tear — pain and weakness that arrived gradually, without a clear injury, because the damage had been building inside the shoulder for months or years before symptoms became impossible to ignore.
This guide explains what the rotator cuff is, why it tears, what the symptoms mean, and what treatment looks like at Pure Ortho Hospitals, Sainikpuri, Hyderabad.
What Is the Rotator Cuff?
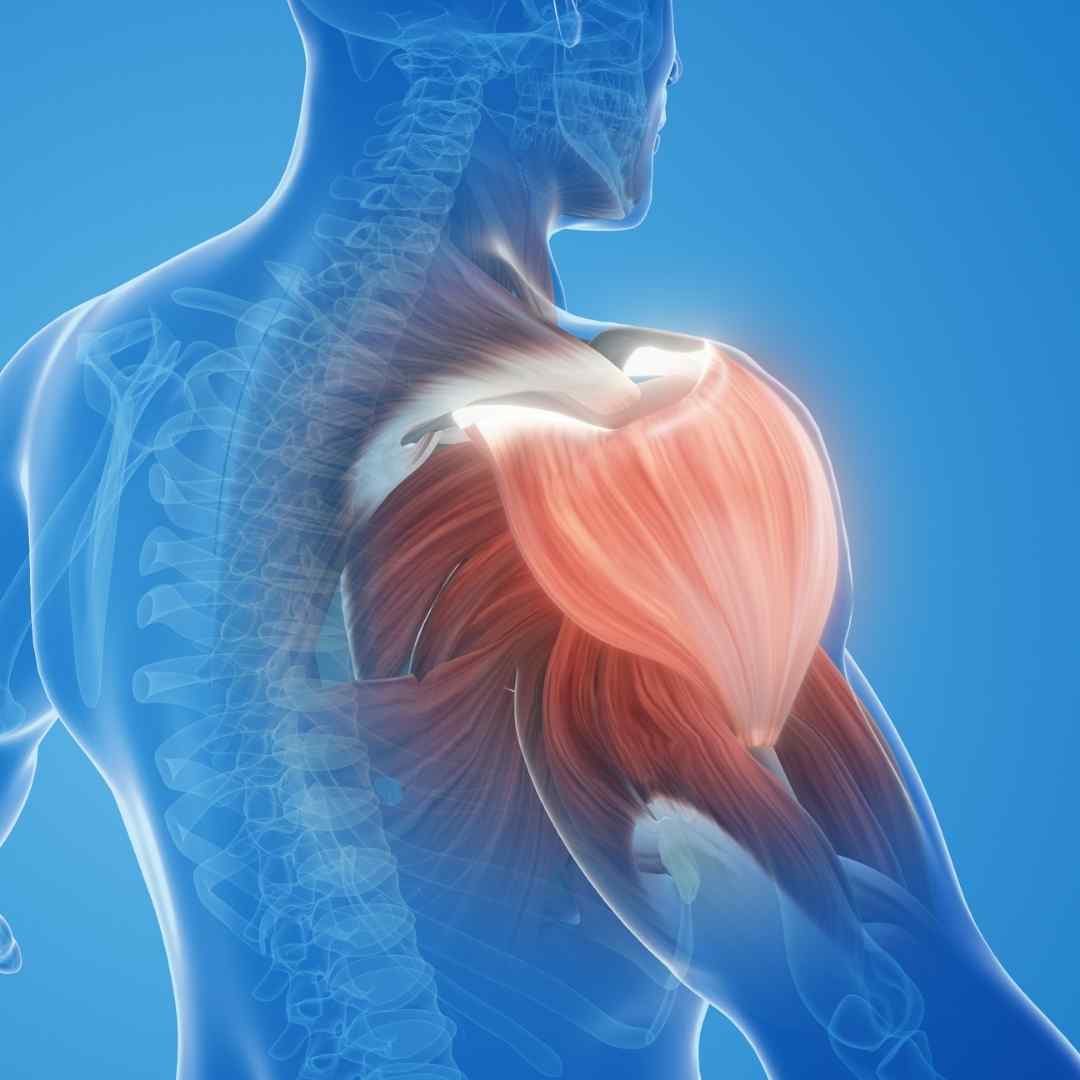
The rotator cuff is a group of four muscles and their tendons that surround the shoulder joint, holding the head of the upper arm bone (humerus) securely in the shallow shoulder socket. It allows the shoulder to move through its remarkable range of motion while keeping the joint stable — a balance between mobility and stability that no other joint in the body achieves to the same degree.
Supraspinatus
Runs along the top of the shoulder blade through a narrow space under the acromion bone. Initiates arm lifting. Its position makes it especially prone to compression and reduced blood supply — the primary reason it accounts for the majority of rotator cuff tears.
Infraspinatus
Located on the back of the shoulder blade. Controls external rotation of the arm. Often involved alongside supraspinatus in larger tears.
Teres Minor
Small muscle assisting external rotation. Rarely torn in isolation — usually involved only in extensive tears.
Subscapularis
Located at the front of the shoulder blade. Controls internal rotation. Tears here are less common but significant when present, often from traumatic injury.
Why the Rotator Cuff Tears — Two Different Patterns
Rotator cuff tears fall into two broad categories, and understanding which type you have changes the entire clinical picture — the likely cause, the expected treatment, and the realistic outlook.
Degenerative Tears
The far more common pattern. The tendon weakens gradually over years from reduced blood supply, repetitive overhead strain, and age-related wear. No single injury causes it — symptoms emerge when the weakened tendon finally tears or becomes significantly inflamed. Most common after age 40.
Traumatic Tears
Caused by a specific event — a fall onto an outstretched arm, lifting something unexpectedly heavy, or a sudden forceful pulling motion. Often occurs in a tendon that already had some degenerative weakening, which is why a relatively minor incident can cause a significant tear.
Repetitive Overhead Strain
Common in people whose daily activities or sport involve repeated overhead arm movement — painters, swimmers, those doing repetitive overhead lifting. Cumulative micro-damage over years precedes the tear.
Subacromial Impingement
The supraspinatus tendon gets repeatedly pinched between the humeral head and the acromion bone above it during arm elevation. Chronic impingement is one of the leading contributors to supraspinatus tendon degeneration and eventual tear.
Gym and Weight Training
Overhead pressing, bench press with poor form, sudden heavy lifting without adequate shoulder conditioning, and excessive training volume without recovery are common precipitating factors — particularly in lifters with pre-existing tendon changes they were unaware of.
Bone Spurs
Bony growths on the underside of the acromion narrow the space the supraspinatus tendon passes through, increasing friction and accelerating degeneration over time.
Tear Severity — Partial, Full-Thickness, and Massive
Incomplete Tendon Damage
Tendon fibres are damaged but the tendon is not completely severed. Often manageable without surgery. May progress to full tear if untreated and the aggravating activity continues.
Complete Tendon Rupture
The tendon is torn completely through, separating from its bone attachment or splitting fully. Causes more significant weakness. Treatment depends on size, patient age, and activity demands.
Multiple Tendons Involved
Two or more rotator cuff tendons are torn, often with significant retraction. Most challenging to repair surgically. Requires specialist assessment for the most appropriate reconstructive approach.
Symptoms of a Rotator Cuff Tear
Pain with Overhead Movement
Reaching up to a shelf, washing hair, or putting on a shirt becomes painful or difficult
Night Pain
Pain that is worse lying on the affected shoulder, frequently disrupting sleep
Arm Weakness
Difficulty lifting the arm, particularly against resistance, or a sense the arm is "giving way"
Crackling Sensation
Crepitus — a crackling or popping sensation when moving the shoulder in certain directions
Gradual Onset Without Injury
Many degenerative tears present with pain that built up over weeks or months with no specific triggering event
Difficulty with Daily Tasks
Combing hair, reaching behind the back, lifting grocery bags — function that was previously unnoticed becomes noticeably affected
Right shoulder pain without injury and left shoulder pain without injury are both extremely common search terms — because this presentation, with no clear traumatic cause, is exactly how the most frequent type of rotator cuff tear shows up. If your shoulder pain started without an obvious cause and has not improved with rest, it warrants evaluation rather than continued self-management.
How Rotator Cuff Tears Are Diagnosed
Diagnostic process at Pure Ortho Hospitals, Sainikpuri
- Clinical history — onset, occupation, sport or gym activity, prior shoulder problems
- Physical examination — specific strength tests for each rotator cuff muscle, impingement tests, range of motion assessment
- X-ray — checks for bone spurs, arthritis, and changes to the acromion shape that may contribute to the tear
- Ultrasound — dynamic, real-time assessment of the tendon; useful for confirming tear presence and guiding injections
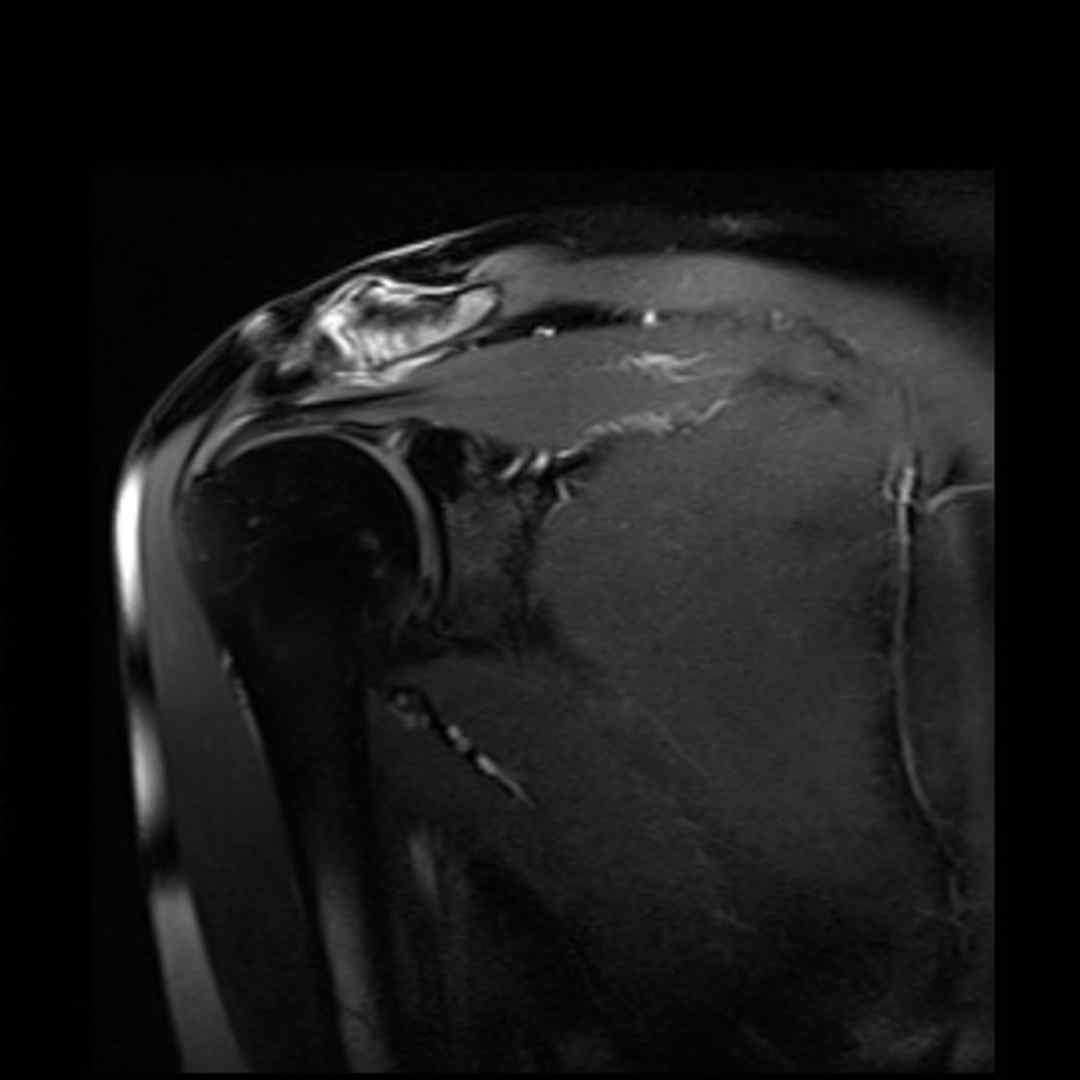
- MRI — the most detailed imaging method; shows the exact tendon involved, tear size, degree of retraction, and muscle quality
Treatment — Conservative First, Surgery When Genuinely Needed
Not every rotator cuff tear requires surgery. Many partial tears and some smaller full-thickness tears, particularly in older or less active patients, are managed successfully without an operation. The decision is based on tear size, the specific tendon involved, the patient's age, activity demands, and response to initial treatment.
Treatment options your specialist may discuss
- Activity modification — avoiding the specific overhead movements aggravating the shoulder
- Physiotherapy — strengthening the surrounding shoulder muscles to compensate, improving scapular mechanics, restoring range of motion
- Anti-inflammatory medication — for pain and inflammation control during the acute phase
- Corticosteroid injection — targeted injection into the subacromial space for significant pain limiting rehabilitation
- Platelet-Rich Plasma (PRP) injection — for select partial tears, to support tendon healing biology
- Arthroscopic rotator cuff repair — minimally invasive keyhole surgery to reattach the torn tendon, performed when conservative treatment fails or the tear is significant in younger active patients
- Tendon transfer or reconstruction — for massive, irreparable tears requiring more complex reconstructive techniques
Arthroscopic repair has become the standard approach for surgically treated rotator cuff tears — performed through small incisions with camera guidance, offering less tissue disruption and a more predictable recovery than traditional open surgery.
See a Specialist Without Delay If
- You cannot lift your arm at all following an injury
- Shoulder weakness is significant and getting worse
- Pain has persisted beyond 4-6 weeks despite rest
- There is visible deformity following a fall or accident
Call Pure Ortho Hospitals, Sainikpuri: 8686868208
Meet the Specialists at Pure Ortho Hospitals
Dr. G. Uday Sekhar Reddy
MBBS, MS Ortho, MCh Ortho
Dr. V.S. Abhilash Kumar S
MBBS, MS Ortho, FIJR, FISS (S.Korea, USA) — Clinical Director
Dr. Sai Karthikeya Badri
MBBS, D. Ortho, DNB
Dr. Pudari Manoj Kumar
MBBS, MS Ortho, FIJR, FIRJR
Dr. L. Sreeram
MPT (Ortho), FDOR, MIAP
Dr. L. Sri Dharani
BPT, MIAP, PTOTA (Canada)
Frequently Asked Questions
Other Departments at Pure Ortho Hospitals
Shoulder Pain That Won't Go Away Needs Proper Evaluation
Whether your shoulder pain started with an injury or seemingly out of nowhere, a proper evaluation identifies exactly what is happening. Visit Pure Ortho Hospitals, Sainikpuri, Hyderabad.
Call 8686868208More from Pure Ortho Hospitals
This article is for patient education only. Please consult a qualified orthopaedic surgeon before making any treatment decisions.